
4 Pitfalls Of Poor-Performing Clinical Trial Teams — And How To Prevent Them
By Monica Roy, consultant

The constantly shifting pharmaceutical landscape frequently leads pharma company senior management teams to shift their clinical development strategies in response. These clin dev shifts in turn affect study teams’ operational activities. Some study teams nimbly pivot while others fall further behind their study timeline. Why is this so?
It comes down to the presence or absence of certain study processes and how refined they are. Unfortunately, by the time a trial starts enrolling subjects (i.e., enters study maintenance), it’s usually too late to course correct.
This is because during study maintenance, the cross-functional study team begins executing the processes that were set up during study start-up. As the study recruits more subjects and heads toward data deliverables, work accelerates. Until the end of the study, on a rolling basis, standard tasks must be carried out, issues are identified and resolved, and upcoming timeline milestones prepared for.
Because of the intensity of this activity (especially on larger, more complex trials), it’s hard for teams to carve out time to focus on processes. This is why teams should:
- set up processes before study maintenance, optimally during study start-up,
- ensure the right processes are in place, and
- ensure the processes are high-quality and set up correctly.
Within the cross-functional study team, creating processes (i.e., “operationalizing” the study) is the main role for the clinical operations group. For that reason, we’ve provided guidance specifically for them.
The guidance herein helps clin ops teams pivot nimbly after unforeseen events (such as strategy shifts or mass layoffs) by avoiding:
- unclear team stakeholders and responsibilities,
- poor communication among team members (cross-functional team, senior management, CRO, vendors, etc.),
- poor alignment in strategy and in timeline among team members, and
- little to no onboarding for new team members.
Unclear Team Stakeholders And Responsibilities
Before tackling communication, clin ops teams must determine who must be communicated with. On very large teams, stakeholders and their responsibilities can get confusing. However, two simple spreadsheets are sufficient for tracking members and responsibilities, so long as they are maintained in real time (usually by a dedicated clinical trial assistant (CTA)) and shared with the entire cross-functional team. These provide a foundational reference for everyone, including people outside of the study team and new study team members.
The first spreadsheet should include the following contact information for the internal study team, relevant internal senior management, vendors, and CRO(s):
- full name
- email address
- time zone
- title (This is usually enough for experienced users to understand a cross-functional team member’s responsibilities, but if needed, a high level “responsibilities” column also can be added to the spreadsheet.)
- company name (e.g., sponsor, vendor, CRO)
- active (yes/no). Certain vendor stakeholders are no longer active after the vendor start-up phase, so this column will allow users to filter them out.
The second spreadsheet should include only the internal study team clinical operations information:
- full name
- detailed study responsibilities (including maintenance of these two spreadsheets)
A simplified RACI (Responsible/Accountable/Consulted/Informed) project management tool format works well here.
Poor Communication Among Team Members
Now that study stakeholders have been identified and organized, clin ops teams must decide on communication channels and rhythms. The main channels for any cross-functional study team are study meetings, high-level study emails, and chat.
Study Meetings
Meetings get a bad rap across many industries, but they are the foundation of effective communication within a highly collaborative, cross-functional team.
The clin ops team should schedule or collaborate with other stakeholders to schedule standard recurring meetings on a frequency that meets the study’s current needs. These meetings include vendor meetings (if needed), data management/cleaning meetings, supply chain meetings, and a protocol deviations quarterly review.
The meetings should also have the right attendees, such as the program management team, study management team, clin ops teams (internal), and other teams as deemed appropriate.
It’s also important to prevent or remove unnecessary meetings so that stakeholders can better register what is communicated during the necessary meetings. Some examples of unnecessary meetings include:
- “pre” and “post” meetings to prep for and analyze other meetings,
- ad hoc meetings to make a decision or explain a scenario that are simple enough to be done via email,
- meetings where a large group of people review a plan or other document together, which can easily be done via email or SharePoint,
- meetings that don’t need to be attended by clin ops (e.g., legal document reviews), and
- meetings where the decision maker does not attend.
Unnecessary meetings are indicative of an unclear meeting purpose, an unclear (or even no) meeting agenda (with attendees veering off topic and needing further meetings to actually make the decision in question), no action items or accountabilities documented at the end of meeting, and lack of overall study strategy or lower-level strategies. Clin ops can avoid unnecessary ad hoc meetings by:
- assessing if the meeting is critical toward the study’s critical path,
- assessing if the meeting should instead be an email or phone call,
- pushing back (respectfully) on invites from other stakeholders or asking what the meeting’s purpose and intended outcome are, and
- always including meeting purpose/agendas/minutes. Agendas and minutes need not always be formal. Sometimes they can just be a bulleted email to attendees.
High-level Study Emails
There’s an interesting inverse relationship between emails and meetings. It’s important to have enough of the “right” meetings. This is because insufficient meetings result in under communication, which triggers the sending of too many emails. However, in certain cases, informational emails must be sent to supplement meetings, either to provide detail not covered during a meeting or provide updates between meetings. Clin ops teams should establish up front the type and recurrence of informational emails such as:
- study enrollment updates
- study timeline updates
- study data cleaning updates
- new team member announcements
- previous member departures and replacements
Chat (Microsoft Teams, Slack, etc.)
Chats can be in a private group, 1:1, or within channels.
Regardless of format, chats should be used solely for ad hoc communication that supplements the two methods above.
Slack and Teams channels can be used effectively as file repositories and to document critical project information and decisions, but this requires a well thought out application policy that details these processes. Therefore, we recommend that most companies and clinical trial teams use chat applications solely for ad hoc, real-time communication instead of anything more elaborate.
Misalignment Among Team Members
After establishing communication channels, teams must ensure that the right information is presented and discussed. All meeting and email content should be driven by the overall study strategy and timeline agreed upon with senior management and the related critical path. Here’s an example of how a clin ops team can efficiently communicate and execute a strategy shift from senior management:
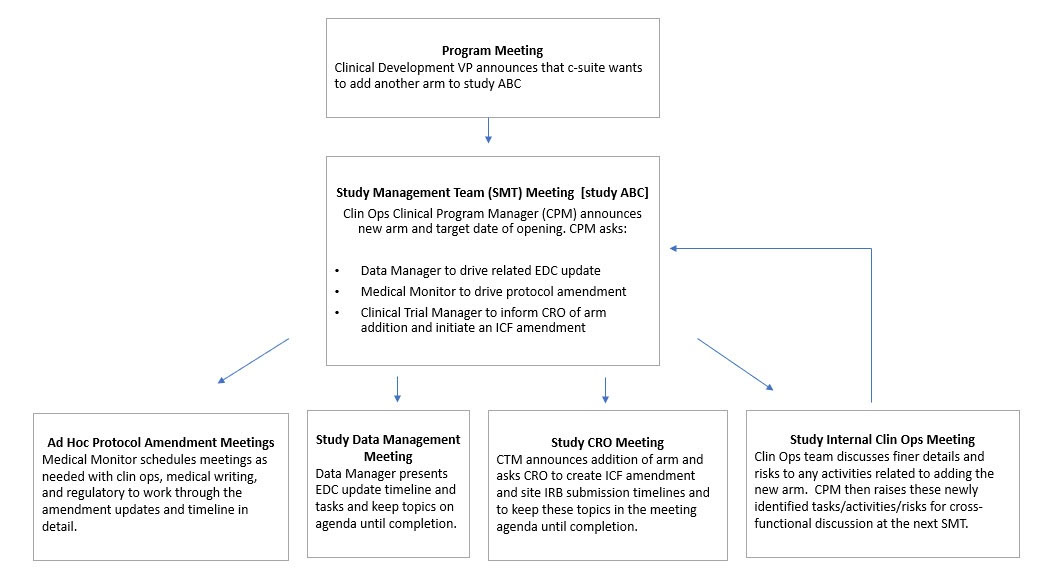
In this way, everything is driven by clear, comprehensive communication at the SMT, which then kicks off smaller tasks and activities to more targeted meetings and interactions. Relevant asks/activities/risks from the smaller meetings that need to be raised cross-functionally are then proposed at the SMT, and the cycle continues.
Little To No Onboarding For New Team Members (Especially In Clin Ops)
At first, team member onboarding may seem unrelated to flexibility or nimbleness. However, it is key. When new members are brought on with adequate onboarding (and shadowing time, if possible), there is a smooth transfer of knowledge and responsibilities that enables the continuity of the study timeline. At a minimum, onboarding should include:
- introduction of the new team member to all study stakeholders they will interact with and a request to include them in all relevant meetings and communications
- team review
- protocol training
- study history, overview, and status review
- timeline review
- responsibilities review
- tools, documents, and shared drive review
When there is little to no onboarding, team members must learn and execute their role simultaneously, which takes longer and is more error prone. This may also lead to the new team members not fully understanding their responsibilities, which, depending on their level of seniority, can put the study timeline at risk.
These issues with little to no onboarding are compounded when a team member joins the team shortly before a large milestone (e.g., data deliverable) or after a strategy shift. In fact, companies with a lot of strategy shifts tend to have high turnover as people who seek stability decide to leave. For these companies, it’s even more important to have decent onboarding. Sometimes a team member leaves before their replacement is hired or identified. In these cases, onboarding should still occur, ideally by a legacy team member who has in-depth study knowledge.
At the end of the day, a team that is progressing while accountable and aligned is more flexible and efficient than one that is not.
About The Author:
 Monica Roy is a consultant and founder of a SaaS company with a clinical operations workflow automation tech platform, as well as an industry consultant. Monica has 20 years of experience working in clinical operations, primarily in oncology. She has led Phase 1 to 3 global trials across small and large pharma companies, with a focus on effectively leveraging process and technology to improve team efficiency and outcomes. Prior to that, she worked in preclinical research at UCSF, which resulted in publication authorships in the journals Neuron, Endocrinology, and others.
Monica Roy is a consultant and founder of a SaaS company with a clinical operations workflow automation tech platform, as well as an industry consultant. Monica has 20 years of experience working in clinical operations, primarily in oncology. She has led Phase 1 to 3 global trials across small and large pharma companies, with a focus on effectively leveraging process and technology to improve team efficiency and outcomes. Prior to that, she worked in preclinical research at UCSF, which resulted in publication authorships in the journals Neuron, Endocrinology, and others.